How do health care professionals diagnose the problem?
Diagnosis begins with a complete history and physical examination. Your physiotherapist at Eastwood Physiotherapy will ask questions about where precisely the pain is, when the pain began, what you were doing when the pain started, and what movements aggravate or ease the pain. As mentioned above, extrinsic factors such as training history as well as type of footwear are important for us to inquire about. The history alone will often lead your physiotherapist to the suspicion of patellar tendonitis.
Next your physiotherapist will do a physical examination of the knee and entire lower extremities. They will palpate, or touch, around the knee and particularly along the patellar tendon to determine the exact location of pain. Your physiotherapist will look for the individual intrinsic factors mentioned above, such as alignment, flexibility and joint laxity that may be affecting your knee. They may want to look at how you stand, your foot position, or watch you walk, squat, or jump. Your physiotherapist in Edmontonwill also check the strength and lengths of the muscles surrounding and affecting the knee joint such as the quadriceps, hamstrings, calves, hip flexors and buttocks muscles. All of these muscles, if weak or tight, can contribute to the forces applied to the knee joint and contribute to the development of patellar tendonitis. Providing resistance while you straighten your knee generally reproduces the pain associated with patellar tendonitis so this will also be tested. Lastly, your physiotherapist will assess the stability of the knee joint to determine if the laxity of the ligaments and tissues surrounding the knee joint are contributing to the problem.
Often patellar tendonitis can be positively diagnosed from the history and physical examination and does not require further investigations. At times, however, further diagnostic tests may be required to either confirm or rule out the diagnosis, or to determine if there are any micro tears in the tendon that may be limiting the tendon from healing as expected. Tests such as ultrasonography or magnetic resonance imaging (MRI) may be used in these cases. Ultrasound uses sound waves to detect tendon tears. MRIs use magnetic waves (rather than X-rays) to create pictures that look like slices of the knee. Normal MRIs do not require any needles or special dyes and are painless. These pictures show the soft tissues of the body. Usually, this test is done to look for other injuries such as tears in the quadriceps. It is also used, however, to identify tears in the patellar tendon and can also confirm inflammation in the area.
If your physiotherapist determines that it would be useful in your case to obtain an ultrasound or MRI, they will inform you of the quickest and most appropriate method of obtaining the investigation.
Eastwood Physiotherapy provides services for physiotherapy in Edmonton.
 The large quadriceps muscle ends in a tendon that inserts into the tibial tubercle, a bony bump at the top of the tibia just below the patella. This is called the infrapatellar tendon or patellar tendon. Another tendon, the quadriceps tendon, attaches from the quadriceps muscle into the top of the patella. These two tendons, together with the patella, are called the quadriceps mechanism.
The large quadriceps muscle ends in a tendon that inserts into the tibial tubercle, a bony bump at the top of the tibia just below the patella. This is called the infrapatellar tendon or patellar tendon. Another tendon, the quadriceps tendon, attaches from the quadriceps muscle into the top of the patella. These two tendons, together with the patella, are called the quadriceps mechanism.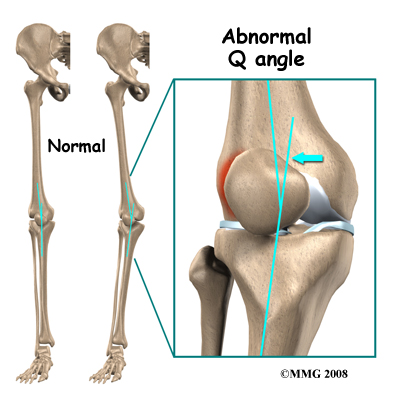 Intrinsic factors such as age, flexibility, and joint laxity are also important. Misalignment of the foot, ankle, and leg can play a key role in tendonitis. Factors such as a flat foot position, tracking abnormalities of the patella, rotation of the tibia (tibial torsion,) and a leg length difference can create increased and often uneven load on the quadriceps mechanism that can contribute to the development of patellar tendonitis.
Intrinsic factors such as age, flexibility, and joint laxity are also important. Misalignment of the foot, ankle, and leg can play a key role in tendonitis. Factors such as a flat foot position, tracking abnormalities of the patella, rotation of the tibia (tibial torsion,) and a leg length difference can create increased and often uneven load on the quadriceps mechanism that can contribute to the development of patellar tendonitis.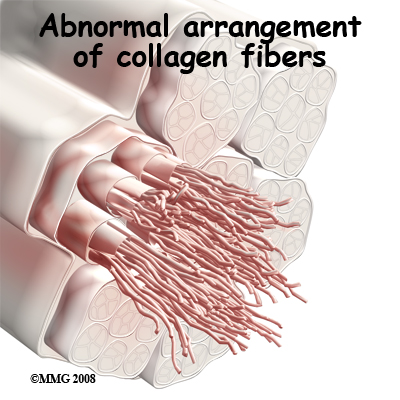 Strength of the patellar tendon is in direct proportion to the number, size, and orientation of the collagen fibers that make up the tendon. Overuse is simply a mismatch between load or stress on the tendon and the ability of that tendon to distribute the force. If the forces placed on the tendon are greater than the strength of the structure, then injury can occur. Pain develops when microtrauma to the musculotendinous junction develops due to the repetitive pull during knee flexion and extension. Tissue breakdown then occurs triggering an inflammatory response that leads to tendonitis.
Strength of the patellar tendon is in direct proportion to the number, size, and orientation of the collagen fibers that make up the tendon. Overuse is simply a mismatch between load or stress on the tendon and the ability of that tendon to distribute the force. If the forces placed on the tendon are greater than the strength of the structure, then injury can occur. Pain develops when microtrauma to the musculotendinous junction develops due to the repetitive pull during knee flexion and extension. Tissue breakdown then occurs triggering an inflammatory response that leads to tendonitis. What does patellar tendonitis feel like?
What does patellar tendonitis feel like?