What treatment options are available?
Nonsurgical Treatment
Treatment begins with conservative (non-operative) care. This may include rest and/or changes in weight-training activities and techniques. Avoiding over-training and smoking are two very effective ways to prevent this condition. Over-training adds too much stress to the bone, which can contribute to rapid bone breakdown. Smoking decreases the amount of oxygen available to the bones and tissues and thus creates a less resilient tissue. If you do develop weightlifters shoulder, take quick steps to modify your weightlifting techniques and avoid over-training.
One of our physiotherapists at Eastwood Physiotherapy can help you with advice for activity modification and specific strength training tips for this problem. For example, if you narrow your hand spacing on the barbells this takes the stress off the distal clavicle. Stopping your bench press two inches above the chest also decreases the stress on the distal clavicle. Some lifters place a two-inch folded towel on the chest as a reminder of when to stop.
The power clean or power jerk can also be modified. Don't rack the bar (lift the bar and let it rest on the clavicles or deltoids.) Start with the elbows even with, or above your shoulders and lift. This eliminates the power pull. If you do develop weightlifters shoulder then certain activities such as bench press, dips, and push-ups should be avoided for a while to allow healing. Applying ice massage and taking ibuprofen after each workout or exercise session can help.
If you work directly with a personal trainer they should also be able to provide tips for proper technique during your actual session to avoid this injury, along with other common weight lifting injuries.
Athletes must be careful to follow all recommendations for program modifications. There is a tendency to work through the pain and not really modify the program at all.
In addition to modifying your weightlifting technique, any muscular imbalances around your shoulder should be addressed. Your physiotherapist at Eastwood Physiotherapy will assess the strength of your shoulder, chest and back muscles and determine if any areas are not strong enough or other areas are too strong in comparison to the rest.
Weightlifters are prone to have stronger chest and shoulder muscles than those of the back and posterior shoulder. This imbalance can also contribute to the pressure on the distal clavicle, and the development and lingering pain of weightlifters shoulder. Your physiotherapist will prescribe exercises for you that address any imbalance that is present. Often the exercises we prescribe to correct the imbalance will be similar to the ones that you have been doing at the gym already, and can be done with barbells or light weights, but the ratio of exercises that are done for your chest and anterior shoulder is often much less than what we will prescribe for your back and posterior shoulder. Proper technique is also of utmost importance so we will ensure you use good technique before using weights that are heavy.
Imbalances around the shoulder can also occur because of tissues that are too tight.
Your physiotherapist will also assess which muscles you should be stretching in your particular case to address any imbalances. Again, weightlifters have a tendency to be tight around the chest and anterior shoulder, but these areas will be individually assessed by your physiotherapist to decide whether this is the case for you in particular.
In addition to addressing any strength and range of motion imbalances around your shoulder, rehabilitating the shoulder from this injury requires exercises that address your shoulder proprioception. Shoulder proprioception is the unconscious ability for you to know where your shoulder is in space during everyday, as well as sporting activities.
Gaining adequate shoulder proprioception, especially of the shoulder blade, is a extremely important component of any shoulder rehabilitation program because the shoulder is a very mobile joint that easily becomes pinched or impinged if it is not moving well. This impingement is even greater when under load, such as lifting weights.
Your physiotherapist will spend time teaching you proper shoulder proprioception and prescribe specific exercises for this, such as gentle rowing with a light band, or overhead reaching and pulling while you focus on the position of your shoulder blade.
At Eastwood Physiotherapy we also encourage you to maintain your body’s overall fitness level even if you have had to take a break from your regular weightlifting or substantially decrease the amount you are doing. A stationary cycle, elliptical, or step machine can all be useful ways to maintain your cardiovascular health while you recover from your injury. If you are a runner, you may be able to continue running as long as the pumping action of the arms does not induce your shoulder pain.
With conservative care and the proper rehabilitation routine outlined by one of our physiotherapists at Eastwood Physiotherapy, you will likely feel a lessening of painful symptoms until you are pain free. As you improve, your physiotherapist will help you gradually resume all activities without bringing back the problem.
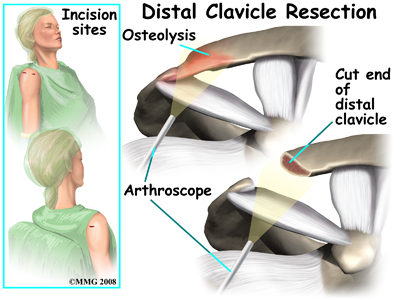
If the pain does not resolve with conservative care, or you are not able to resume your normal activities, surgical intervention, which removes, or ‘resects’ a portion of the end of the clavicle bone may be required. In cases such as these, your physiotherapist will refer you on to seek the opinion of an Orthopaedic Surgeon.
Interestingly, some athletes who progress through the pain without activity modification, may, in a way, perform surgery on themselves. In this form of self-surgery, as the injury progresses the clavicle will resect on its own as the bone breaks down and breaks off. Unfortunately, there will still be an inflammatory response with increased symptoms that still sets you back in your program. In addition, if the body doesn’t resorb the broken off bone, surgery may be required anyways to extract it. It is our recommendation at Eastwood Physiotherapy that a period of activity modification in addition to an appropriate rehabilitation program is adhered to.
Eastwood Physiotherapy provides services for physiotherapy in Edmonton.
 Welcome to Eastwood Physiotherapy's guide to Weightlifter's Shoulder (Distal Clavicular Osteolysis)
Welcome to Eastwood Physiotherapy's guide to Weightlifter's Shoulder (Distal Clavicular Osteolysis)
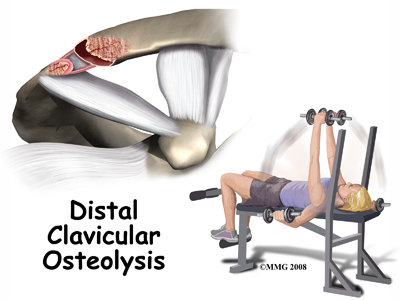
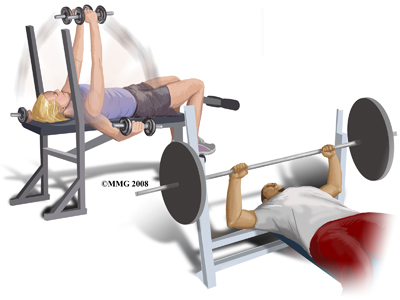 Repetitive trauma or stress from training and lifting causes tiny fractures of the distal end of the clavicle bone. Excessive traction on the AC joint from bench presses or chest fly exercises occurs when the elbows drop below or behind the body. This places the shoulders in a position of excess extension. As the bone does not have a chance to heal before the next training session begins, the bone actually starts to dissolve.
Repetitive trauma or stress from training and lifting causes tiny fractures of the distal end of the clavicle bone. Excessive traction on the AC joint from bench presses or chest fly exercises occurs when the elbows drop below or behind the body. This places the shoulders in a position of excess extension. As the bone does not have a chance to heal before the next training session begins, the bone actually starts to dissolve.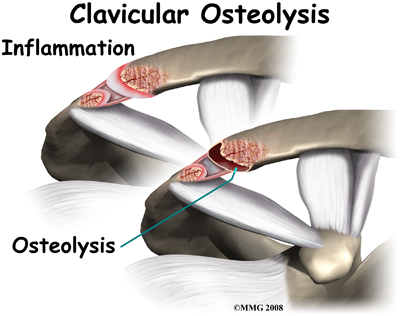 In studying this injury, there is evidence that the body tries to heal the fractured bone but the bone dissolves or is resorbed by the body instead. A network of blood vessels forms in the area during the attempted healing process. Chronic inflammation with scar tissue called fibrosis is commonly found when tissue from the area is examined under a microscope.
In studying this injury, there is evidence that the body tries to heal the fractured bone but the bone dissolves or is resorbed by the body instead. A network of blood vessels forms in the area during the attempted healing process. Chronic inflammation with scar tissue called fibrosis is commonly found when tissue from the area is examined under a microscope.