What should I expect during my rehabilitation?
You will probably wear a knee brace for up to six weeks after surgery to protect the knee joint as you recover. Your stitches will normally be removed in 10 to 14 days. Although the time required for rehabilitation varies, recovery after a tibial osteotomy typically takes two to three months.
During your recovery period, you should use your walker or crutches as instructed by our physiotherapist. If you had a closing wedge osteotomy, you probably won't have to limit how much weight you place on your foot. But with an opening wedge procedure, you'll need to protect the healing bone graft by only placing the toes of the operated leg on the floor when you walk. Your surgeon will take a follow-up X-ray to see when the graft is safe for you to begin putting more weight down when you walk. This is usually six to eight weeks after surgery.
Your physiotherapist can begin assisting you with treatment shortly after surgery. Our physiotherapist may use heat, ice, or electrical stimulation if you have swelling or pain. We may also use hands-on stretches and show you exercises to improve knee range of motion. Then strength exercises will be used to address key muscle groups including the buttock, hip, thigh, and calf muscles. Endurance can be achieved through stationary biking, lap swimming, and using an upper body ergometer (upper cycle).
Our physiotherapists sometimes treat patients in a pool. Exercising in a swimming pool puts less stress on the knee joint, and the buoyancy lets you move and exercise easier. Once you've gotten your pool exercises down and the other parts of your rehab program advance, we may instruct you in an independent program.
When you are safe in putting full weight through the leg, our physiotherapist can choose several types of balance exercises to further stabilize and control your knee.
Finally, we will utilize a select group of exercises to simulate day-to-day activities, such as going up and down steps, squatting, rising on your toes, and bending down. Other specific exercises may then be chosen to simulate work or hobby demands.
Many patients have less pain and better mobility after a tibial osteotomy procedure. Our physiotherapist will work with you to help keep your knee joint healthy for as long as possible. This may require that you adjust your activity choices to keep from placing too much strain on your knee.
At Eastwood Physiotherapy, our goal is to help you improve knee range of motion, maximize strength, and improve your ability to do your activities. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
Eastwood Physiotherapy provides services for physiotherapy in Edmonton.
Portions of this document copyright MMG, LLC.
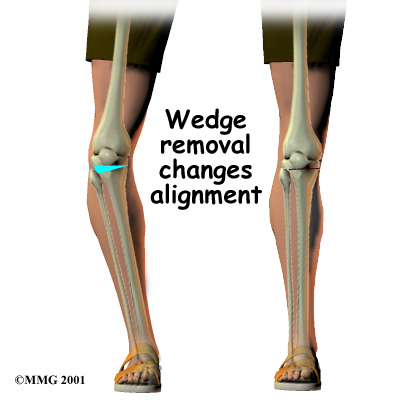
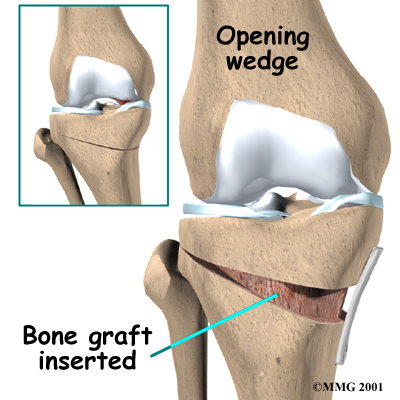
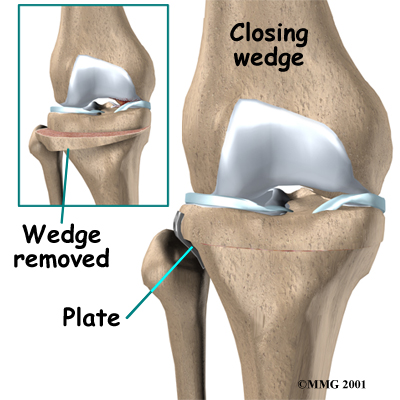 There are two methods to realign the knee joint. One involves taking out a wedge of bone; the other involves adding a wedge of bone. Any operation for cutting through a bone is called an osteotomy. In a closing wedge osteotomy, the surgeon cuts though the tibia on the lateral side, removes a wedge of bone, and pins the open edges together. In an opening wedge osteotomy, the surgeon cuts though the tibia on the medial side and opens a wedge, adding a bit of bone graft to hold the wedge open.
There are two methods to realign the knee joint. One involves taking out a wedge of bone; the other involves adding a wedge of bone. Any operation for cutting through a bone is called an osteotomy. In a closing wedge osteotomy, the surgeon cuts though the tibia on the lateral side, removes a wedge of bone, and pins the open edges together. In an opening wedge osteotomy, the surgeon cuts though the tibia on the medial side and opens a wedge, adding a bit of bone graft to hold the wedge open.