What happens during the operation?
Reconstruction
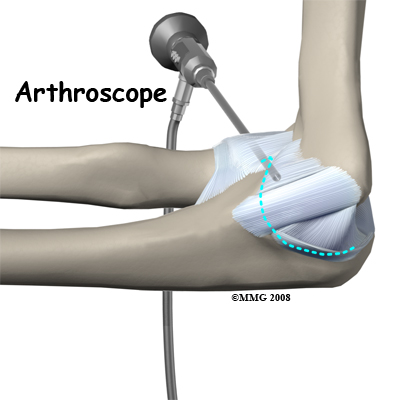
If you are having problems that may be coming from inside the joint, such as arthritis and loose bodies, your surgeon may perform an arthroscopy before the actual reconstruction procedure is done. During this procedure, a small TV camera is inserted into the elbow joint through two or three small (1/4 inch) incisions. Using special instruments your surgeon will be able to evaluate the joint, remove any loose bodies and bone spurs that may be causing problems. Arthroscopy is not always necessary.
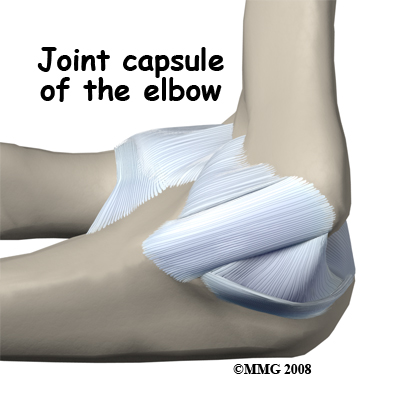
 The reconstruction is performed though an on the medial (inside) side of the elbow joint. The damaged ulnar collateral ligament along the medial (inside) of the elbow is replaced with a tendon harvested from somewhere else in the body. The tendon graft can come from the patient's own forearm, hamstring, knee, or foot. This is called an autograft.
The reconstruction is performed though an on the medial (inside) side of the elbow joint. The damaged ulnar collateral ligament along the medial (inside) of the elbow is replaced with a tendon harvested from somewhere else in the body. The tendon graft can come from the patient's own forearm, hamstring, knee, or foot. This is called an autograft.
Over the years the way that surgeons perform this operation has improved. In the early days, the muscles on the inside of the elbow joint and forearm (the flexor muscles) were completely detached from the humerus and the ulnar nerve was re-routed from its normal position in the cubital tunnel on the back side of the elbow. This was done to be able to see the joint and protect the nerve. As surgeons have understood this problem more completely, these two parts of the operation have been eliminated. Now, the flexor muscles are not detached, but are split and retracted to allow the surgeon to see the areas of the elbow joint required to perform the operation successfully. The ulnar nerve is re-routed only if the patient is having symptoms of ulnar nerve damage before the operation is performed. These improvements have resulted in a less invasive procedure with a decreased rate of complications.
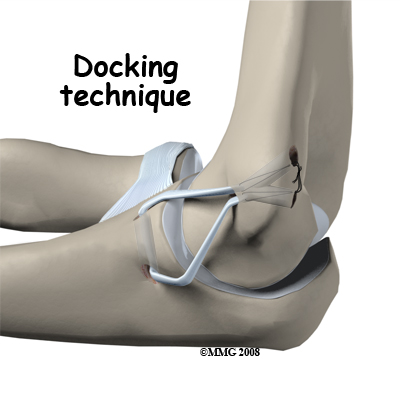
One common technique used to replace the damaged ulnar collateral ligament is called the docking technique. The surgeon drills two holes in the ulna and three in the medial epicondyle ( the small bump of bone on the inside of the elbow at the end of the humerus). The two holes in the ulna form a tunnel that the tendon graft will be looped through. The three holes in the medial epicondyle form a triangle. The bottom hole will be bigger than the top two holes, so that the surgeon can slide the end of the tendon graft into the bottom hole. The two top holes are used to pull the tendon graft into the tunnel using sutures that are attached to the graft and threaded through the two holes.
After the tendon is harvested, sutures are attached to both ends. The tendon is looped through the lower tunnel formed in the ulna, and stretched across the elbow joint. The two sutures attached to the ends of the graft are threaded into the larger bottom tunnel in the medial epicondyle and each is threaded out one of the upper, smaller holes.
 Using these two sutures, the surgeon pulls the end of the graft farther into the upper tunnel until the amount of tension is correct to hold the joint in position. The surgeon carefully puts the elbow through its full arc of motion and readjusts the tension on the sutures until he is satisfied that the proper ligamentous tension is restored. The two sutures are tied together to hold the tendon graft in that position.
Using these two sutures, the surgeon pulls the end of the graft farther into the upper tunnel until the amount of tension is correct to hold the joint in position. The surgeon carefully puts the elbow through its full arc of motion and readjusts the tension on the sutures until he is satisfied that the proper ligamentous tension is restored. The two sutures are tied together to hold the tendon graft in that position.
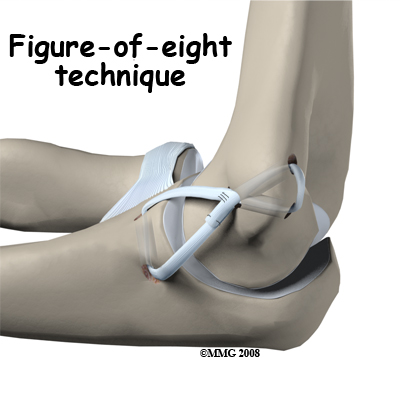
Another common technique to reconstruct the ulnar collateral ligament is the technique. In this technique, the tendon graft is threaded through two pairs of holes - two drilled in the medial epicondye and two in the ulna. The graft is looped through the holes in a figure of eight fashion. The two ends of the tendon are sutured to the tendon itself.
If there is any concern that the ulnar nerve has been stretched and damaged due to the instability (as mentioned above), it may be re-routed so that it runs in front of the elbow joint rather than through the cubital tunnel in the back of the elbow. The incision is sutured together and the elbow is placed in a large bandage and splint.
There are several newer techniques being developed that hopefully will make the procedure even less invasive while retaining the success that the docking technique has enjoyed.